
Features of a droopy tip include inferior rotation of the tip and an acute nasolabial angle. Droopy tips can result from intrinsic or extrinsic factors or a combination thereof. The intrinsic factors are a long, lateral crus, a cephalic orientation of the lateral crus, or a weak, medial crus. The extrinsic factors responsible for droopy tips are tension nose (oversized septal cartilage), long upper lateral cartilage, or a weak tip or thick tip skin being pulled down by gravity.
The choice of surgical technique for the correction of a droopy tip depends on its etiology.
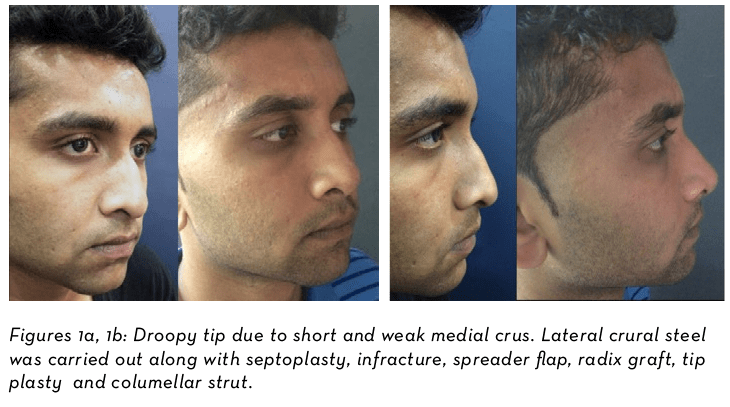
Lateral crural steal, lateral crural overlay¹ and tongue-in-groove² techniques are useful when a droopy tip is due to an intrinsic factor. Similarly, resection of oversized septum, long upper lateral cartilage and strengthening of the medial crura by columellar strut may be chosen depending on the extrinsic factor that is responsible for the droopy tip. Certain ancillary measures are also taken to aid the superior rotation of tip. Keeping in mind the tripod analogy, the medial crus fixation suture is used along with an interdomal stitch to allow the paired lower lateral cartilage to rotate in unison. Cephalic trim of lateral crus and/or excision of the scroll area may be required to create the space for superior rotation of tip. Lateral crural steal pulls the medial part of lateral crus into the middle crus by means of horizontal mattress suture. This, in addition to rotating the tip, also increases its projection. Lateral crural steal is indicated in droopy tips due to weak medial crura, evident by its buckled appearance (Figures 1a, 1b).